
The shoulder is one of the most complex and mobile joints in the human body. However, it is also highly susceptible to injury, wear-and-tear, and chronic pain. For millions of people, shoulder pain is not just a temporary inconvenience but a debilitating condition that limits daily activities, professional performance, and overall quality of life. In this post, we’ll explore the conditions that can cause shoulder pain, along with the spectrum of potential treatments.
Key Takeaways
- Shoulder pain can originate from a variety of structures, including tendons, bursae, cartilage, bone, and nerves.
- Many shoulder pain conditions are successfully managed with non-surgical methods like rest, physical therapy, anti-inflammatory medications, and targeted injections.
- Advanced surgical options can be effective for conditions that fail conservative treatment or involve significant structural damage.
The Anatomy Behind Shoulder Pain
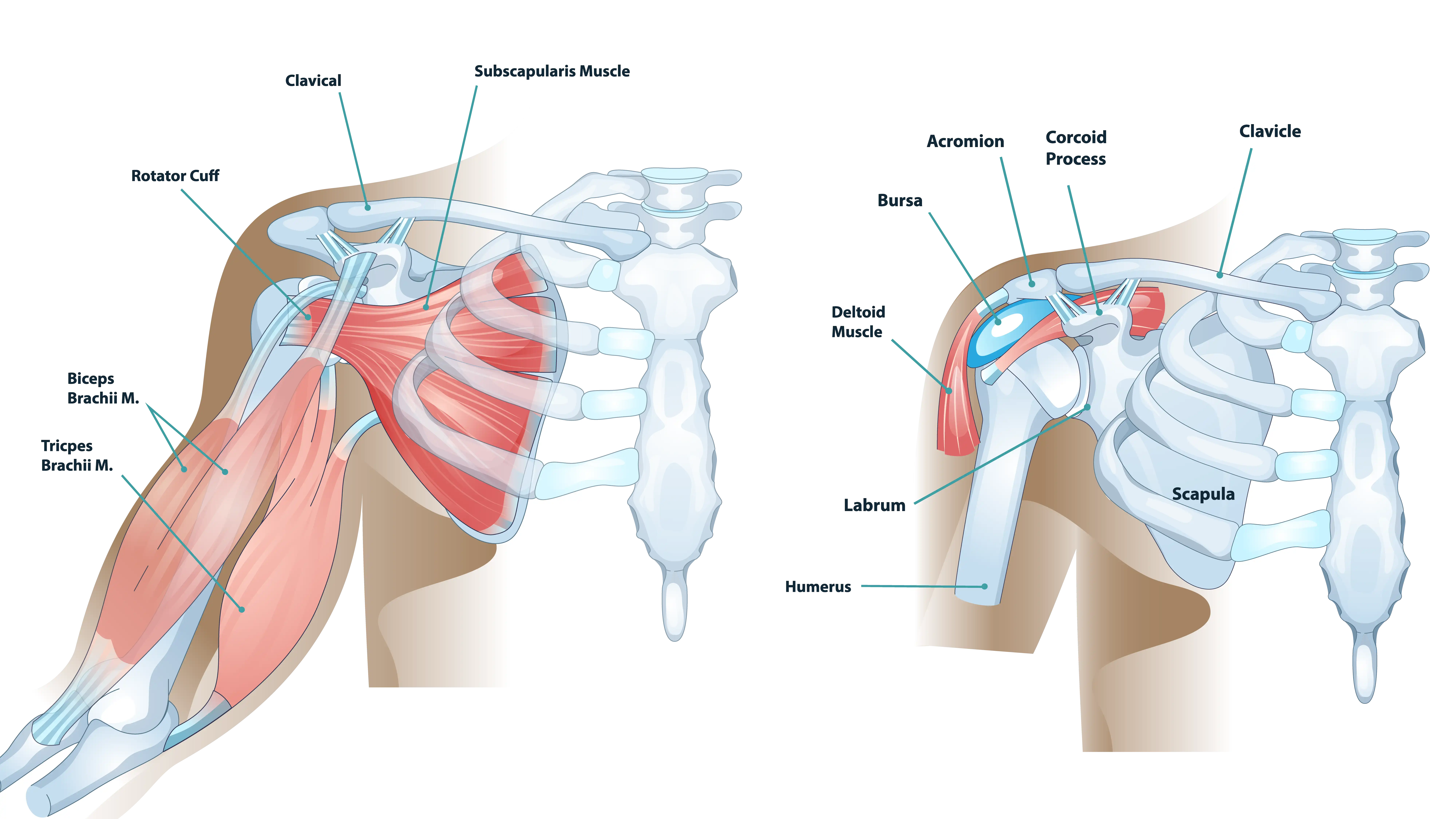
The shoulder joint is comprised of three bones: the humerus (upper arm bone), the scapula (shoulder blade), and the clavicle (collarbone). The primary joint, the glenohumeral joint, is a ball-and-socket mechanism that provides the shoulder’s remarkable range of motion. This incredible mobility, however, comes at the expense of inherent stability, making the surrounding soft tissues (the capsule, ligaments, and rotator cuff) essential for keeping the joint centered and functional.
Common Causes of Shoulder Pain
When any of the shoulder structures become irritated, injured, or weakened, shoulder pain can develop. In the following subsections, we’ll review some of the common reasons individuals experience shoulder pain.
Rotator Cuff Injuries
The rotator cuff is a group of four muscles and their tendons that surround the shoulder joint, providing stability and allowing the arm to rotate and lift. Injuries to this structure are perhaps the most common cause of shoulder pain.

- Tendinitis and Impingement Syndrome: Rotator cuff tendinitis is the inflammation of the tendons, often due to repetitive overhead activities or poor shoulder mechanics. This frequently coexists with shoulder impingement syndrome, where the tendons are pinched between the acromion (the top part of the shoulder blade) and the head of the humerus, particularly when the arm is lifted. This narrowing of the subacromial space can be exacerbated by bone spurs or the shape of the acromion itself.
- Rotator Cuff Tears: These range from partial-thickness tears (damage to the tendon but not completely through it) to full-thickness tears. Tears are typically caused by acute trauma (e.g., a fall) or chronic degeneration (wear-and-tear) over time.
Instability and Dislocation
Shoulder instability occurs when the head of the humerus is forced out of the shoulder socket (the glenoid). A shoulder dislocation is an acute event where the ball completely separates from the socket. Repeated dislocations or chronic looseness of the joint, often due to damaged ligaments and capsule, can lead to chronic instability.
Arthritis
Arthritis is the breakdown of the smooth articular cartilage that cushions the bones in the joint. In the shoulder, this most commonly affects the glenohumeral joint or the acromioclavicular (AC) joint. There are different arthritic conditions, including osteoarthritis, rheumatoid arthritis, and post-traumatic arthritis.
Frozen Shoulder (Adhesive Capsulitis)
This condition involves the thickening and tightening of the capsule of connective tissue that encases the shoulder joint. It progresses through three distinct stages: freezing (painful, progressive loss of motion), frozen (stiff but less painful, motion severely restricted), and thawing (slow return of motion).
Other Common Causes
- Bursitis: Inflammation of the bursa, a small fluid-filled sac that acts as a cushion between the bones and the tendons/muscles. It often occurs alongside impingement syndrome.
- Biceps Tendinitis and Tears: Inflammation or tearing of the long head of the biceps tendon, which runs through the shoulder joint. A complete tear can result in a visible bulge in the upper arm.
- AC Joint Separation: Injury to the ligaments connecting the clavicle and the acromion, frequently caused by a fall directly onto the shoulder.
- Referred Pain: Pain felt in the shoulder that actually originates from another area.
Treatments From Conservative Care to Advanced Reconstruction
The treatment for shoulder pain is highly individualized and depends on the diagnosis, the severity of the condition, the patient’s age, activity level, and overall health goals. An experienced shoulder surgeon can evaluate the condition and help guide the most appropriate treatment path.
Conservative (Non-Surgical) Management
Many shoulder conditions respond well to a structured, non-surgical approach.
Rest and Activity Modification
Patients may be encouraged to avoid activities that provoke pain, particularly repetitive overhead motions. This does not necessarily mean complete immobilization, which can lead to stiffness, but rather adjusting lifestyle and work habits, like using adaptive equipment or changing technique during sports or work. Ice packs applied for 15–20 minutes several times a day may help reduce inflammation and pain, especially after activity, while heat can relax tight muscles and improve blood flow.
Medications and Injections
Non-steroidal anti-inflammatory drugs (NSAIDs), whether over-the-counter or prescribed, can help reduce pain and inflammation when used under medical guidance. In some cases, a corticosteroid injection may be recommended. These injections deliver powerful anti-inflammatory medication directly into the affected area, offering short-term relief. Platelet-rich plasma (PRP) therapy, a regenerative treatment where concentrated platelets are injected into the injury site, may also be an option for some conditions.
Physical Therapy (PT)
A customized physical therapy program focuses on restoring range of motion, strengthening key muscle groups, and improving posture and body mechanics. Therapy usually begins with gentle passive motion before progressing to active and strengthening exercises for both the rotator cuff and the muscles around the shoulder blade. Therapists also may help patients correct posture and movement patterns during everyday tasks or sports to prevent re-injury.
Advanced (Surgical) Interventions
When conservative treatments fail to provide relief after a dedicated course of several months, or when the initial injury is severe, surgical intervention may be necessary. The goal of surgery is to restore the structural integrity of the joint and reduce pain.
Shoulder Arthroscopy: The Minimally Invasive Standard
Shoulder arthroscopy uses a small camera and specialized instruments inserted through tiny incisions to visualize and repair structures in and around the joint. This minimally invasive approach generally causes less trauma to surrounding tissues and may support a faster recovery. Common arthroscopic procedures include rotator cuff repair, labral repair for instability (reattaching the torn labrum to prevent dislocations), and subacromial decompression for impingement (removing bone spurs and inflamed tissue to create more space for the tendons).
Shoulder Replacement
For advanced arthritis or massive, irreparable rotator cuff tears, shoulder replacement surgery provides a possible solution. In an anatomic total shoulder arthroplasty, both the humeral head and the socket are replaced with smooth artificial components, typically when the rotator cuff is intact. In a reverse total shoulder arthroplasty, the ball and socket positions are reversed, allowing the deltoid muscle to lift the arm in place of a damaged rotator cuff.
The Post-Surgical Journey: Commitment to Rehabilitation
A typical post-surgical rehabilitation protocol is structured into distinct phases, each with specific goals and restrictions. Timelines and steps may vary depending on the condition, the chosen treatment option, and individual health factors.
Phase I (Protection and Passive Motion): Initially, the goal is to protect the surgical repair and prevent stiffness. The arm is kept in a sling, and motion is strictly passive, meaning the therapist or the patient’s other arm moves the operative arm without the use of the repaired muscles.
Phase II (Active Motion and Early Strengthening): Once the surgeon determines the repair is stable enough, the patient may begin active range of motion exercises, using their own muscles to move the arm. Light, isometric strengthening exercises may be introduced.
Phase III (Advanced Strengthening and Endurance): The focus often shifts to restoring strength, power, and endurance. Resistance exercises with bands, light weights, and functional movements may be utilized to prepare the shoulder for daily activities and work.
Phase IV (Return to Activity): This final phase frequently involves highly specific, sport- or work-related training. For athletes, this includes a gradual return to throwing, swinging, or contact activities.
Preventing Shoulder Pain: Long-Term Strategies for Shoulder Health
While some injuries are unavoidable, many chronic shoulder problems are the result of cumulative microtrauma and poor biomechanics. Adopting preventative strategies can be helpful for maintaining long-term shoulder health.
- Maintain Good Posture: Keep the shoulders back and down, your monitor at eye level, and your elbows close to your body. Take frequent stretch breaks during desk work.
- Strengthen Scapular and Rotator Cuff Muscles: Focus on endurance-based exercises like rows, banded external rotations, and “Y” or “T” raises to build shoulder stability.
- Use Proper Lifting and Throwing Mechanics: Keep objects close to your body when lifting, and when applicable, generate power from your core and legs rather than solely the shoulder.
- Warm Up Before Activity: Begin any workout, sport, or physical task with 5–10 minutes of gentle cardio and dynamic shoulder movements (arm circles, band work) to increase blood flow and tissue elasticity.
- Gradually Increase Activity Intensity: Avoid sudden increases in workout load or repetitions. Progressive overload, slowly increasing resistance or duration, helps the tendons and muscles to adapt safely.
- Pay Attention to Early Pain Signals: Stop activities that cause pain, rest, and seek medical advice if discomfort lasts more than a week or strength suddenly declines.
Summary: Taking Control of Your Shoulder Health
By understanding the underlying causes of shoulder pain, from tendinitis and impingement to complex rotator cuff tears and advanced arthritis, patients can partner with their orthopedic specialist to develop a targeted treatment plan. The path to relief often begins with conservative measures, placing an emphasis on physical therapy and activity modification. For those whose structural damage is too significant, modern advancements in minimally invasive shoulder arthroscopy and shoulder replacement techniques aim to restore function and eliminate chronic pain for many patients.
Frequently Asked Questions
What is the difference between a total shoulder replacement and a reverse shoulder replacement?
Total shoulder replacement is typically used when the rotator cuff is intact and functional. It mimics the natural anatomy (ball on humerus, socket on scapula). Reverse shoulder replacement may be preferred when the rotator cuff is severely damaged or non-functional. It reverses the ball and socket positions, allowing the large deltoid muscle to lift the arm and compensate for the damaged rotator cuff.
When should I see a doctor for my shoulder pain?
Consider seeking professional orthopedic care immediately if you experience sudden, severe pain, an inability to move your arm, a visible deformity around the shoulder joint, or pain that persists for over a week. Listen to your body’s signals to determine if it is time to consult a doctor.
What is “rotator cuff tear arthropathy”?
This is a severe, specific type of shoulder arthritis that develops when a massive, long-standing rotator cuff tear is present. Because the rotator cuff is responsible for centering the humeral head in the socket, its absence can cause the humeral head to migrate upward, rubbing against the acromion.
