
For many individuals, a persistent ache on the inner side of the elbow can become a significant source of frustration. This condition, known as golfer’s elbow or medically as medial epicondylitis, affects the tendons that connect the forearm muscles to the bone at the elbow joint. Many individuals may wonder, “What causes golfer’s elbow?” While the name suggests a link to the golf course, the reality is that this painful condition can affect anyone who engages in repetitive arm, wrist, or hand motions.
Key Takeaways
- • Golfer’s elbow is generally not caused by a single event, but rather by repeated stress and strain on the forearm flexor tendons.
- • Many activities, including throwing, racket sports, and various occupational tasks, can lead to this injury.
- • Factors like age, poor technique, muscle weakness, and smoking may increase your susceptibility.
- • Proper technique, conditioning, and early rest can be helpful for avoiding the onset or recurrence of symptoms.
The Anatomy of the Injury: A Look Inside the Elbow
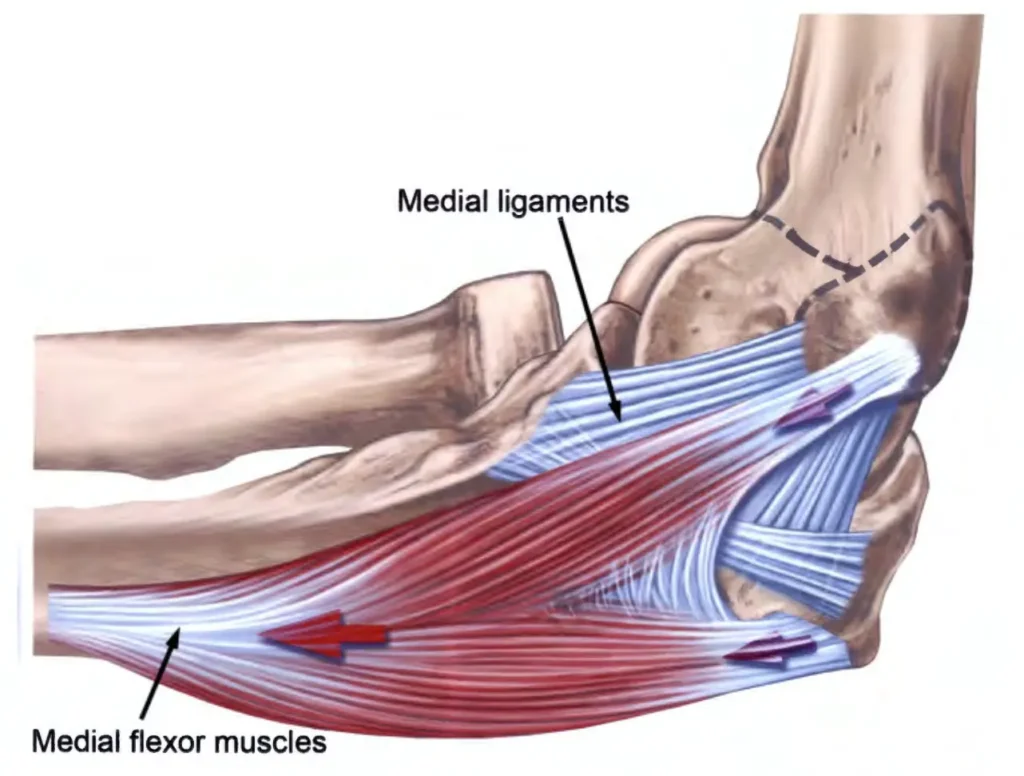
To understand what causes golfer’s elbow, we must first examine the anatomy of the elbow joint. The elbow is a hinge joint that allows for flexion and extension, as well as rotation of the forearm.
The medial epicondyle, a bony bump on the inside of the elbow, serves as the anchor point for a group of muscles known as the flexor-pronator mass. These muscles are responsible for several movements. They allow you to flex your wrist (bend it forward). They also enable you to pronate your forearm (turn your palm downward). Furthermore, they are heavily involved in gripping actions. The tendons of these muscles converge at the medial epicondyle.
When you repeatedly use these muscles, especially with force or resistance, the tendons may be subjected to strain. Over time, this repeated stress may exceed the tendon’s capacity to repair itself.
The Primary Mechanism: Repetitive Strain and Microtrauma
Golfer’s elbow is usually a cumulative overuse condition, developing slowly over weeks or months. Each time the forearm muscles contract forcefully, a pulling force is exerted on the tendons. This force is concentrated at the medial epicondyle. Activities that require repeated wrist flexion and forearm pronation are particularly stressful. Think of the motion involved in hammering, throwing a baseball, or swinging a golf club.
With repeated, forceful contractions, the collagen fibers within the tendon begin to sustain microscopic tears, or microtrauma. Normally, the body’s natural healing process repairs these small injuries. However, when the activity is constant and the rest periods are insufficient, the rate of damage surpasses the rate of repair. This imbalance leads to a cycle of injury and incomplete healing.
The tendon tissue begins to break down and degenerate. This degenerative process resulting from overuse is known as tendinosis. This weakened tendon may then be less able to handle the normal stresses of daily life.
Activities That Place the Elbow at Risk
While the name is a convenient label, medial epicondylitis is not exclusive to golfers. A wide array of sports and occupational activities can create the necessary conditions for this injury to develop. The common thread among these activities is the requirement for forceful, repetitive use of the wrist flexors and forearm pronators.
Sports-Related Causes
Golf: The golf swing is a classic example of the mechanism of injury. The condition is often triggered by the powerful wrist snap required at impact. Additionally, hitting a “fat” golf shot where the club strikes the ground before the ball can transmit a sudden, violent shock up the arm. This sudden jolt can be particularly damaging to the already stressed tendons. Poor swing mechanics, such as an overly tight grip or excessive wrist action, may also increase the risk.
Throwing Sports: The late cocking and acceleration phases of the throwing motion involve intense, rapid contraction of the forearm muscles. This repetitive, high-velocity stress may lead to microtrauma at the medial epicondyle.
Racket Sports: Tennis players, while more commonly associated with lateral epicondylitis (tennis elbow), can also develop the medial form. This is especially true if they use a heavy top-spin forehand. The wrist snap and forearm rotation needed for top-spin may overload the medial tendons. Using a racket that is too heavy or has a grip that is too small may also contribute to the problem.
Weightlifting: Individuals who lift weights, particularly those who focus heavily on bicep curls or exercises involving a tight, sustained grip, may be at risk. Improper technique during exercises like wrist curls, where the wrist is repeatedly flexed against heavy resistance, can strain the medial epicondyle.
Occupational and Daily Life Causes
Many other activities involve the same mechanics. These activities often require prolonged, repetitive gripping or twisting motions.
- • Manual Labor: Carpenters, plumbers, and mechanics frequently use tools that require a strong, sustained grip. Repetitive hammering, turning wrenches, or using screwdrivers can place constant stress on the forearm tendons.
- • Assembly Line Work: Workers performing repetitive tasks, such as packing, sorting, or using small hand tools, may develop the condition.
- • Computer Use: While less common, prolonged and improper use of a computer mouse or keyboard may contribute. An awkward wrist position or excessive gripping of the mouse can place strain on the flexor tendons over the course of a workday.
Lifestyle and Biological Risk Factors
While repetitive motion is the direct cause, several other factors may predispose an individual to developing medial epicondylitis. These factors often relate to the body’s ability to handle stress and repair tissue damage.
Age: The condition most commonly affects adults but can occur at any age. As we age, the blood supply to our tendons may decrease. This can slow down the natural healing and repair processes. Tendons also tend to lose some of their elasticity over time. This makes them potentially more susceptible to degenerative changes.
Smoking: Tobacco use has been identified as a possible risk factor for various tendinopathies. Nicotine and other chemicals in tobacco smoke may impair blood flow. This reduced circulation can limit the delivery of oxygen and nutrients necessary for tendon repair. Smoking may also interfere with the production of healthy collagen.
Diabetes: Individuals with diabetes may have a higher incidence of tendon and joint problems. Poorly controlled blood sugar levels can affect the structure and metabolism of collagen. This may make the tendons more brittle and less resilient to repetitive stress.
Prevention and Early Intervention Strategies
Understanding what causes golfer’s elbow naturally leads to strategies for prevention. In some cases, individuals may help reduce their likelihood of developing this condition.
Biomechanical Adjustments
• Technique Correction: Athletes can work with a coach or professional to ensure proper form.
• Ergonomic Review: For occupational causes, an ergonomic assessment of the workspace may be beneficial.
• Equipment Check: Ensure that sports equipment is correctly sized and weighted.
Conditioning and Strengthening
• Warm-up and Stretching: Before engaging in any strenuous activity, a thorough warm-up is essential. Gentle stretching of the forearm flexors and extensors can prepare the tendons for the load they are about to bear.
• Progressive Strengthening: A targeted exercise program can help strengthen the forearm muscles. This increases their endurance and ability to absorb force.
• Cross-Training: Maintaining overall upper body strength, including the shoulder and rotator cuff, can help stabilize the arm. A strong shoulder and core can reduce the reliance on the smaller forearm muscles to generate power.
Summary
Medial epicondylitis, or golfer’s elbow, is a common and often painful condition. The answer to what causes golfer’s elbow is a combination of factors. The primary cause is the chronic, repetitive microtrauma to the flexor-pronator tendons at their attachment point on the medial epicondyle. This may be compounded by various functional and systemic risk factors.
While the condition can be frustrating, it is important to remember that it is frequently treatable. If you are experiencing persistent pain on the inside of your elbow, consider consulting with an experienced elbow specialist. A professional evaluation can help confirm a diagnosis and develop a personalized treatment plan aimed at restoring the strength and function of your elbow.
Frequently Asked Questions
Is golfer’s elbow always caused by playing golf?
No, while golf is a common trigger, the condition can be caused by any activity that involves forceful, repetitive use of the wrist flexor and forearm pronator muscles. This includes throwing sports, racket sports, and various manual labor jobs like carpentry or plumbing.
How long does it typically take for golfer’s elbow to heal?
The healing time can vary significantly depending on the severity and how long the condition has been present. Mild cases might improve within a few weeks with rest and conservative treatment. However, chronic or severe cases may require several months of dedicated physical therapy and treatment to fully resolve.
Is surgery necessary to treat golfer’s elbow?
Surgery is rarely necessary for golfer’s elbow. The vast majority of cases respond well to non-surgical treatments. These typically include rest, physical therapy, bracing, and sometimes injections. Surgery is usually reserved for patients whose symptoms are severe and have failed to improve after several months of comprehensive, non-operative treatment.
